
When Testosterone Takes a Dive: Understanding the Basics
Male hypogonadism is a medical condition where the body doesn’t produce enough testosterone, affecting up to 38% of men over age 45. If you’re researching this condition, here’s what you need to know:
- Definition: A clinical syndrome combining symptoms with testosterone levels below 300 ng/dL
- Types: Primary (testicular failure) or Secondary (pituitary/hypothalamic issue)
- Common symptoms: Fatigue, low libido, erectile dysfunction, decreased muscle mass, increased body fat
- Diagnosis: Requires at least two morning blood tests showing low testosterone
- Treatment options: Lifestyle changes, testosterone replacement therapy, medications that stimulate natural production
“Many people shrug off the symptoms associated with low testosterone as an unpleasant part of getting older. But you should address symptoms that interfere with your quality of life,” notes the Cleveland Clinic.
Male hypogonadism isn’t just about sexual function. It affects your energy, mood, body composition, and even long-term health risks including osteoporosis and cardiovascular disease.
As a man ages, testosterone naturally declines about 1% per year after age 30. However, when levels drop significantly below normal range, causing noticeable symptoms, that’s when medical intervention might be needed.
I’m Len Berkowitz, a physician assistant with over 17 years of experience treating male hypogonadism at the Center for Men’s Health Rhode Island, where we specialize in comprehensive evaluation and personalized treatment plans for men experiencing symptoms of low testosterone.
What Is Male Hypogonadism? Definitions, Types & Prevalence
When we talk about male hypogonadism, we’re describing more than just a low testosterone number. It’s actually a clinical syndrome where symptoms and blood tests both point to testosterone deficiency. According to the American Urological Association, the official cutoff is less than 300 ng/dL, though some doctors use 250 ng/dL as their threshold for diagnosis.
This condition can affect men at any age, from teenagers to seniors, and it comes in several different forms that help us understand what’s really happening in the body.
Male hypogonadism classification map
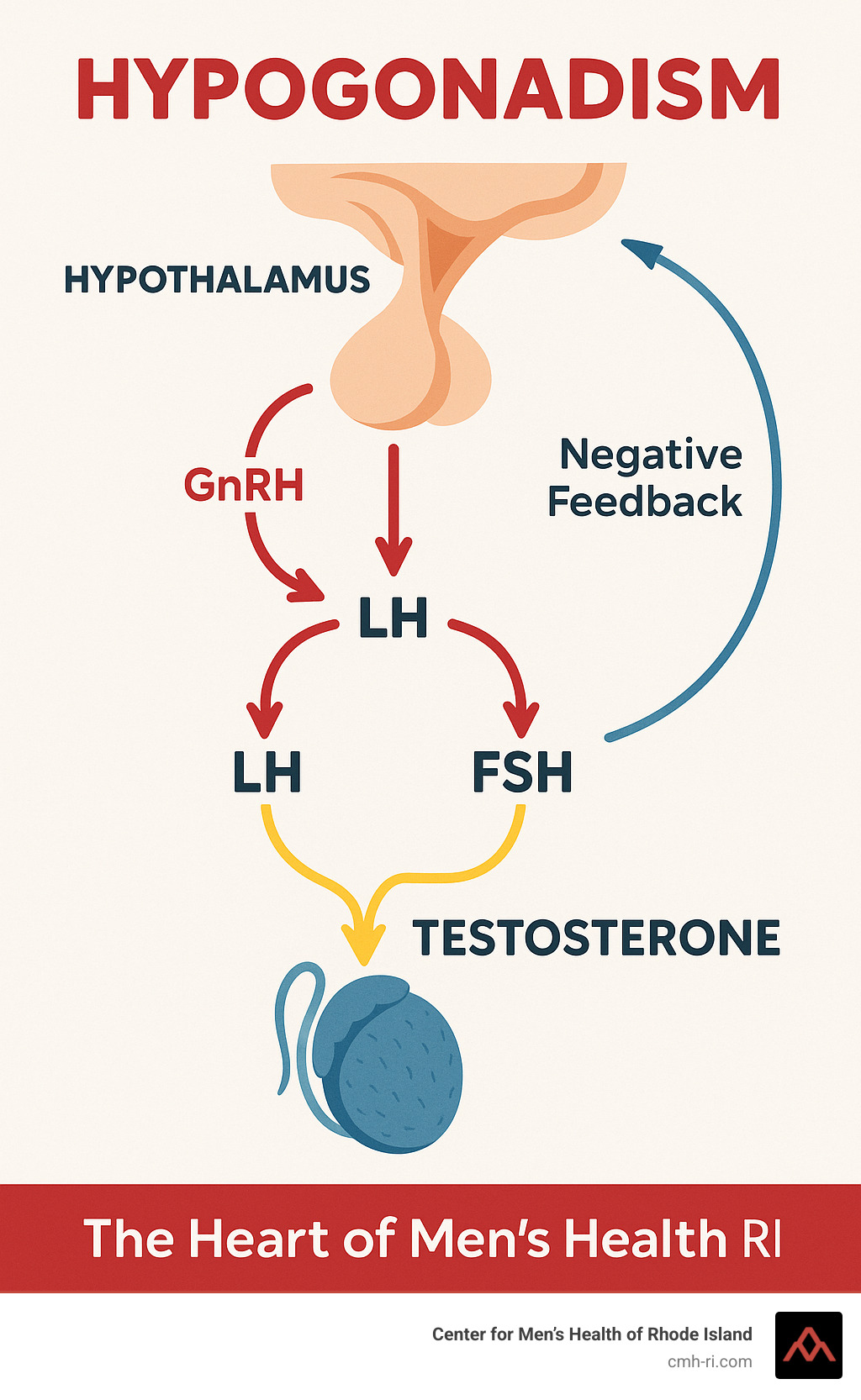
Think of your body’s testosterone production like a three-part relay race. When something goes wrong, it can happen at different points in the race:
Primary Hypogonadism is when the problem is with the testicles themselves. Despite getting all the right signals from the brain saying “make testosterone,” the testicles can’t respond properly. Your blood work tells the story—low testosterone levels but high LH and FSH (the signaling hormones), as if your brain is shouting louder and louder at testicles that can’t hear.
Secondary Hypogonadism is when the starting runners (your hypothalamus or pituitary gland) don’t initiate the race properly. They’re not sending the right signals to your testicles. Blood tests show low testosterone with low or normal LH and FSH levels—essentially, the testicles aren’t getting the message to produce testosterone in the first place.
There’s also Compensated or Subclinical Hypogonadism, where your testosterone levels look normal, but your body is working overtime to maintain them—like a car engine that’s revving too high just to maintain normal speed. Your liftd LH levels reveal this hidden struggle.
We also distinguish between Functional and Organic Hypogonadism. Organic causes involve structural problems or genetic issues that may be permanent, while functional causes might be reversible—things like weight gain, certain medications, or chronic stress.
As men age, many experience Late-Onset Hypogonadism (LOH), typically after 40, where testosterone gradually declines alongside specific symptoms.
Epidemiology snapshot
Male hypogonadism is far more common than most people realize:
Between 11.7 and 12.3 new cases develop per 1,000 people each year. When we look specifically at men between 40-79 years old who have both low testosterone and symptoms, the rate sits between 2.1% and 5.7%.
Perhaps most striking is that approximately 35% of men older than 45 have some form of hypogonadism. That’s one in three men in this age group!
The most common genetic cause, Klinefelter syndrome, affects 1 in 500 to 1,000 male births, yet fewer than half of these men ever receive a proper diagnosis.
There’s also a strong connection with other health conditions—30-50% of men with obesity or type 2 diabetes have hypogonadism. This connection works both ways, as low testosterone can contribute to weight gain and insulin resistance, while excess weight can further suppress testosterone.
As research from the Journal of Advanced Pharmaceutical Technology & Research notes, “The prevalence of symptomatic testosterone deficiency is 2.1%-12.8% in middle-aged to older men,” highlighting just how common this condition truly is.
The aging process itself contributes to declining testosterone. Men typically lose about 0.4% of their total testosterone and 1.3% of their free testosterone each year after age 30. This means by age 70, many men have significantly lower levels than they had in their younger years.
For more information on diagnostic thresholds and clinical guidelines, you can refer to the Cleveland Clinic’s comprehensive guide on hypogonadism.
At the Center for Men’s Health of Rhode Island, we recognize that these numbers represent real men experiencing real symptoms—and we’re here to help with a proper diagnosis and personalized treatment approach.
Why Does Testosterone Fall? Causes, Risk Factors & Comorbidities
The story behind falling testosterone levels is both fascinating and complex. While some decline is natural with age, many men experience a more dramatic drop due to specific health conditions or lifestyle factors. Understanding these causes is the first step toward effective treatment of male hypogonadism.
As men age, testosterone naturally decreases by about 0.4% per year after 30. By itself, this gradual decline rarely causes significant symptoms. But when combined with other factors, it can lead to clinically low levels that affect quality of life.
Primary causes checklist
When the problem originates in the testicles themselves, we call it primary hypogonadism. Think of it as the production facility itself malfunctioning.
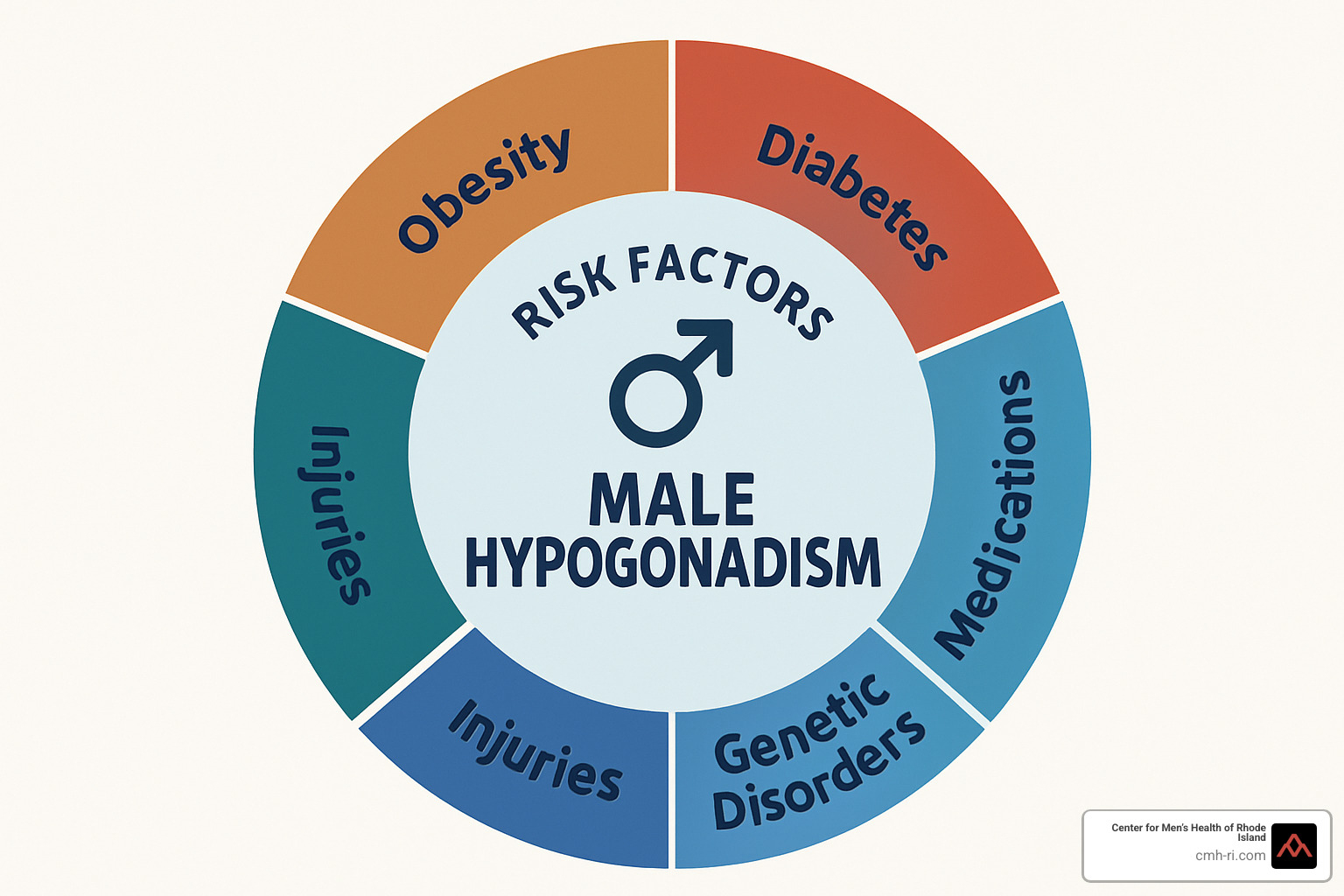
Klinefelter syndrome is the most common genetic cause, affecting about 1 in 500-1,000 men born with an extra X chromosome. Many men don’t even know they have it until they face fertility issues. Other primary causes include undescended testicles that weren’t corrected in childhood, and mumps orchitis – a complication of mumps that can damage testicular tissue.
Physical testicular trauma from sports injuries or accidents can also reduce testosterone production. Less commonly, conditions like hemochromatosis (where excess iron builds up in the body) can damage the testicles over time.
Cancer treatments are another culprit – both chemotherapy and radiation can harm the delicate testosterone-producing cells, sometimes permanently.
Secondary/functional triggers
Secondary hypogonadism happens when the brain’s signaling system fails to properly instruct the testicles. It’s like having a fully functional factory, but the management team isn’t sending proper production orders.
Obesity has emerged as one of the most common causes of low testosterone in modern America. For every point your BMI increases, testosterone typically decreases by about 10 ng/dL. The excess fat tissue converts testosterone to estrogen, creating a hormonal imbalance.
“We often see dramatic improvements in testosterone levels when patients lose just 5-10% of their body weight,” we’ve observed at our Center for Men’s Health of Rhode Island.
Type 2 diabetes and metabolic syndrome frequently go hand-in-hand with low testosterone, creating a vicious cycle – low T leads to more fat storage, which further lowers testosterone. About 17% of men with type 2 diabetes have low testosterone levels.
Sleep apnea disrupts the body’s overnight hormone production, when much of your testosterone is made. Similarly, chronic stress keeps cortisol levels high, which directly suppresses testosterone production.
Certain medications are notorious testosterone-sappers. Opioid painkillers can dramatically reduce levels even after short-term use. Steroids (like prednisone), some psychiatric medications, and treatments for prostate enlargement can all impact testosterone production.
Emerging research has even shown connections between COVID-19 severity and low testosterone levels, though the exact relationship is still being studied.
At the Center for Men’s Health of Rhode Island, we carefully evaluate all these potential causes. Sometimes addressing the underlying condition – losing weight, improving sleep, managing stress, or adjusting medications – can restore testosterone to healthy levels without hormone replacement therapy.
Spotting the Signs & Getting the Right Diagnosis
Have you been feeling unusually tired lately? Or perhaps noticed a drop in your sex drive? These could be more than just signs of a busy life—they might be pointing to male hypogonadism.
Recognizing what low testosterone looks like in your body is the crucial first step toward getting the help you need. Let’s walk through what to watch for and how we diagnose this condition.
Signs and Symptoms
When testosterone levels fall in adulthood, your body sends various signals. You might notice a dramatic drop in your sex drive or difficulty maintaining erections. Many men describe a persistent fatigue that coffee just can’t fix, along with a frustrating loss of muscle despite regular workouts.
Your body composition might change too—more belly fat appearing while your arms and legs seem less defined. Some men experience mood changes, finding themselves irritable or even depressed without obvious cause. Less commonly, you might notice thinning body hair, hot flashes, or even tender, enlarged breast tissue (gynecomastia).
One of our patients, a 61-year-old carpenter named J.H., described his experience perfectly: “I could work, do my job, but would feel exhausted when I came home. I would force myself to exercise at a local club but feel like I’ve lost motivation, and the workouts simply tire me out more.”
If low testosterone begins earlier in life, during adolescence, the signs look quite different. Young men might show delayed puberty with minimal facial hair, a high-pitched voice, less developed muscles, and proportionally longer limbs. In rare cases affecting fetal development, genital abnormalities might be present at birth.

Male hypogonadism diagnosis criteria
Diagnosing male hypogonadism isn’t as simple as a single blood test. We follow a careful process to ensure accuracy:
First, we need to confirm low testosterone with blood tests taken in the morning (between 7-10 AM), when your levels are naturally highest. A single reading below 300 ng/dL isn’t enough—we need at least two low measurements on different days to make a diagnosis.
Your symptoms matter just as much as the numbers. We often use screening questionnaires like the Androgen Deficiency in Aging Males (ADAM) or the Aging Males’ Symptoms scale (AMS) to systematically assess your experience.
To understand what’s causing your low testosterone, we measure other hormones like luteinizing hormone (LH) and follicle-stimulating hormone (FSH). These tell us whether the problem starts in your testicles (primary hypogonadism) or in your brain (secondary hypogonadism).
Sometimes we need to dig deeper with additional tests. We might check your prolactin levels to rule out a pituitary tumor, or iron studies to look for hemochromatosis. If you’re concerned about fertility, a semen analysis helps complete the picture. For men with bone density concerns, we might recommend a DEXA scan, and in cases of secondary hypogonadism, an MRI of the pituitary gland may be necessary.
As one clinical guideline puts it: “Diagnosis requires clinical history, physical exam, morning fasting testosterone tests (repeated), LH/FSH/prolactin assays, SHBG and sometimes imaging or bone density scans.”
Diagnostic workflow
At the Center for Men’s Health of Rhode Island, we take a thorough approach to diagnosing male hypogonadism:
We start with a comfortable conversation about your symptoms, medical history, medications, and lifestyle. Many men find relief just in having someone take their concerns seriously.
The physical examination helps us spot visible signs of low testosterone, from body fat patterns to muscle development. We’ll also check testicular size, which can provide important clues.
Then comes the laboratory testing—those morning testosterone measurements we mentioned, along with related hormones. When needed, we’ll check your free testosterone levels, sex hormone-binding globulin (SHBG), and estradiol.
We’re careful to rule out other conditions that can mimic hypogonadism symptoms. Thyroid disorders, depression, and sleep apnea can all cause similar fatigue and mood changes, so we want to make sure we’re addressing the real issue.
The Mayo Clinic emphasizes that “early detection in boys can help prevent problems from delayed puberty, and early diagnosis and treatment in men offer better protection against osteoporosis and other related conditions.”
Our goal isn’t just to determine if you have low testosterone, but to understand why—because that’s the key to effective treatment. Whether you’re struggling with energy levels, sexual function, or mood changes, we’re here to help you find answers and solutions.
More info about Testosterone Testing
Fixing Low T—Evidence-Based Treatments & Expected Benefits
When you’re diagnosed with male hypogonadism, it’s natural to wonder what comes next. The good news is that several effective treatment options exist, and the right approach for you depends on what’s causing your low testosterone, your age, symptoms, whether you want children, and your overall health picture.
Male hypogonadism treatment options
First things first—sometimes the simplest solutions make a big difference. If you’re carrying extra weight, shedding some pounds can naturally boost your testosterone levels. Regular exercise, especially weight training, can work wonders too. Getting enough sleep (aim for 7-9 hours), managing stress, cutting back on alcohol, and avoiding anabolic steroids and opioids all help support healthy testosterone levels.
As the Endocrine Society points out, “Some causes of hypogonadism like obesity may be reversible without testosterone therapy.” Sometimes addressing these underlying factors is enough to get your testosterone back on track.
When lifestyle changes aren’t cutting it, testosterone replacement therapy (TRT) becomes the main treatment for symptomatic hypogonadism. You’ve got several options here:
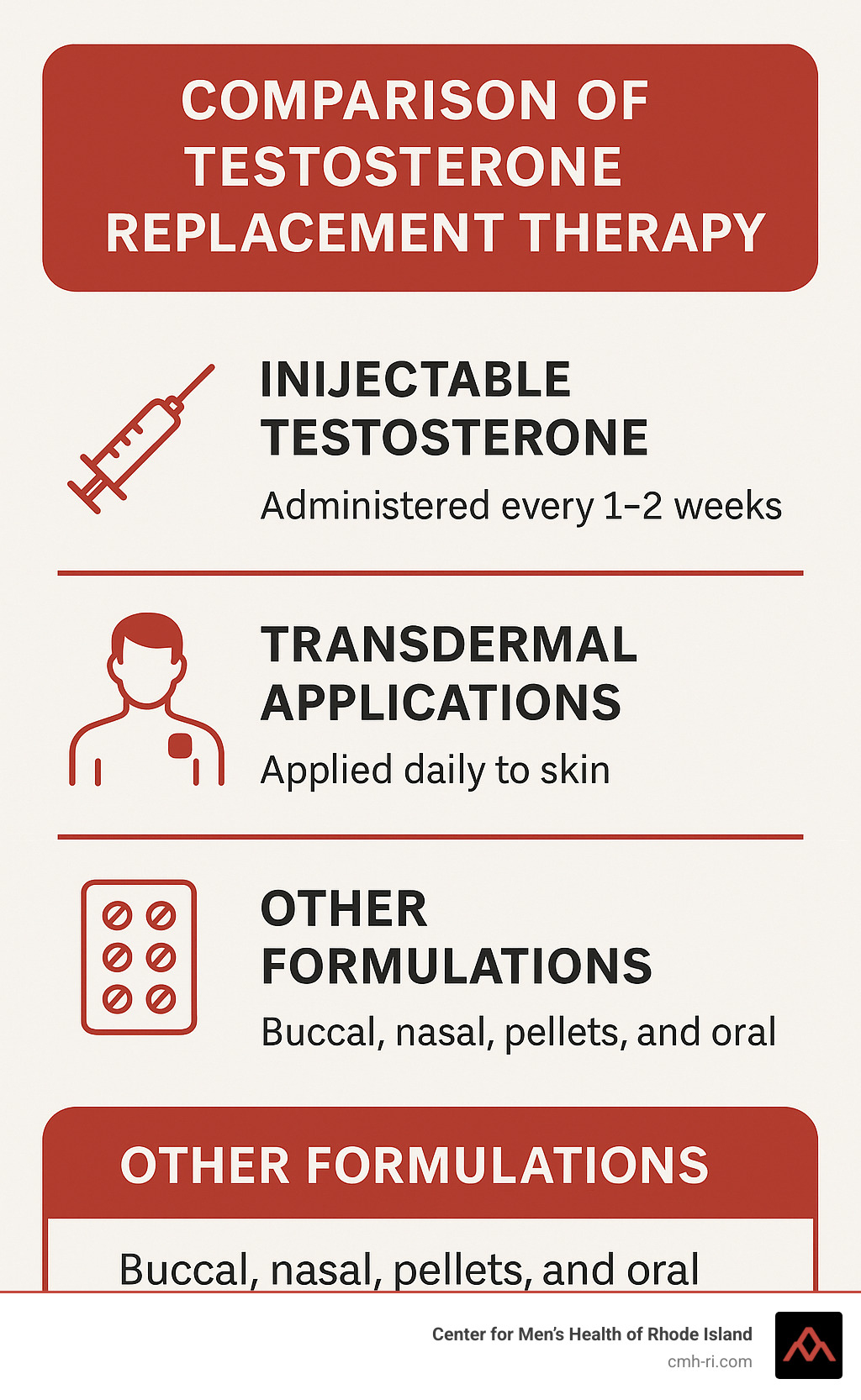
Injectable testosterone gives you flexibility with dosing schedules. The standard versions (cypionate or enanthate) need to be injected every 1-2 weeks, while testosterone undecanoate is a longer-acting option given every 10-14 weeks.
If you’re not a fan of needles, transdermal applications might be your speed. Daily testosterone gels get applied to your shoulders, upper arms, or abdomen, while patches go on your back, abdomen, upper arms, or thighs.
Other options include buccal testosterone (a tablet that sticks to your gum twice daily), nasal testosterone gel (applied inside your nostrils three times daily), subcutaneous pellets (implanted under your skin and lasting 3-6 months), or the newer oral testosterone undecanoate capsules that get absorbed through your lymphatic system.
If you’re hoping to have children, standard testosterone replacement actually works against you by suppressing your body’s natural production. As clinical research cautions, “Testosterone therapy is contraindicated in individuals who desire fertility, as it suppresses gonadotropin and endogenous testosterone secretion as well as spermatogenesis.”
Instead, fertility-preserving treatments like clomiphene citrate stimulate your body’s natural testosterone production. Human chorionic gonadotropin (hCG) mimics LH to boost testosterone production, while FSH therapy combined with hCG helps when sperm production is severely impaired. For hypothalamic hypogonadism, pulsatile GnRH therapy delivered via pump might be recommended.
For more information about erectile dysfunction treatment options that may complement testosterone therapy, you can visit our Erectile Dysfunction services page.
At the Center for Men’s Health of Rhode Island, we don’t believe in one-size-fits-all approaches. We carefully select the most appropriate treatment based on your specific needs and preferences, considering factors like convenience, cost, skin sensitivity, and whether you need steady hormone levels throughout the day.
Expected benefits timeline
When you start testosterone therapy, the benefits unfold gradually, like chapters in a book:
The first few weeks (3-6 weeks) often bring noticeable improvements in sexual desire and function. Many men tell us they feel a positive shift in mood and wellbeing during this time, along with more energy for daily activities.
By the 3-6 month mark (12-24 weeks), you’ll likely see more physical changes. Your muscles may become more defined as you gain lean mass, while stubborn body fat starts to diminish. Many men experience improved insulin sensitivity during this period, and your red blood cell production increases (which we’ll monitor carefully).
The long-game benefits (6-12 months or longer) include increased bone mineral density—important for preventing fractures as you age. The improvements in body composition typically continue, and some research suggests potential reduction in cardiovascular risk factors. Most importantly, many men experience a sustained improvement in overall quality of life.
Research notes that “Testosterone therapy in hypogonadal men improved glycaemic control in some randomized controlled trials,” highlighting benefits beyond just sexual health. The landmark T4DM trial showed that testosterone therapy combined with lifestyle changes reduced progression to diabetes compared to lifestyle changes alone in men with both prediabetes and low testosterone.
It’s important to have realistic expectations about what treatment can do. While many men report significant improvements—sometimes describing it as “getting their life back”—results vary based on age, the cause of your hypogonadism, how long you’ve had symptoms, and your overall health.
At the Center for Men’s Health of Rhode Island, we’ll work closely with you to find the right treatment approach and track your progress, making adjustments as needed to help you feel your best again.
Safety, Fertility & Follow-Up
Treating male hypogonadism effectively means balancing the benefits of therapy with careful monitoring and awareness of potential concerns. While testosterone replacement therapy (TRT) can be life-changing, it’s not simply a matter of “take this and call me in a year.”
Safety Considerations
TRT isn’t right for everyone. Men with certain conditions should avoid testosterone therapy, including those with:
Prostate or breast cancer – testosterone may stimulate growth of these hormone-sensitive cancers
Severe untreated sleep apnea – testosterone might worsen this condition
Uncontrolled heart failure – fluid retention from TRT could exacerbate symptoms
High red blood cell counts (hematocrit above 54%) – testosterone increases red blood cell production, potentially making blood too thick
Plans for fatherhood soon – TRT suppresses sperm production
Severe urinary tract symptoms – may worsen prostate-related urinary issues
Most men tolerate TRT well, but side effects can occur. You might experience acne or oilier skin, mild fluid retention, or breast tenderness. More concerning issues include testicular shrinkage (since your body isn’t working to produce its own testosterone anymore), increased red blood cell count, and reduced fertility.
“Possible side effects include injection-site pain, skin irritation, increased red cell mass (polycythaemia) and prostate enlargement, all monitored by regular blood tests and exams,” explains clinical literature.
The cardiovascular safety of TRT has been the subject of significant debate. The good news is that more recent, high-quality research has largely dispelled earlier concerns. Current evidence suggests:
- No compelling evidence of increased cardiovascular events for most men
- Potential heart benefits for men with metabolic syndrome or diabetes
- Possible reduction in mortality for properly treated hypogonadal men
A comprehensive review concluded: “There is no scientific basis to suggest testosterone therapy increases cardiovascular risk; evidence indicates substantial benefits.”
Regarding prostate health, we now know that TRT doesn’t substantially increase prostate cancer risk as once feared. Still, we carefully monitor prostate health through regular examinations, PSA testing, and evaluation of any new urinary symptoms.

Fertility Considerations
Here’s something many men don’t realize until they’re deep into treatment: testosterone replacement shuts down your body’s natural production of both testosterone and sperm. This creates a paradox – the very treatment that helps restore your masculinity can prevent you from becoming a father.
For younger men or anyone considering future fatherhood, we discuss options like:
Sperm banking before starting TRT – think of it as an insurance policy for your future family
Alternative treatments such as clomiphene citrate or hCG that can improve testosterone while maintaining fertility
Recovery timeline – if you stop TRT to try for pregnancy, fertility typically returns within 3-12 months, though some men may take longer or not fully recover after years of treatment
“Testosterone therapy can improve milder forms of erectile dysfunction and libido in hypogonadal men,” research shows, “but must be balanced against fertility concerns in younger men.”
For more detailed information about free testosterone calculation methods that help guide treatment decisions, you can visit the International Society for the Study of the Aging Male’s free testosterone calculator.
Male hypogonadism follow-up protocol
At the Center for Men’s Health of Rhode Island, we believe proper monitoring makes all the difference between successful therapy and problematic treatment. Our follow-up protocol is thorough and personalized:
First follow-up (3 months after starting):
We’ll check your testosterone levels, aiming for the middle of the normal range – not too high, not too low. We’ll also run a complete blood count to check for increased red blood cells, assess liver function, measure PSA (for men over 40), and most importantly, talk about how you’re feeling.
Ongoing monitoring (6 months, then annually):
We continue checking hormone levels, blood counts, and metabolic markers like cholesterol and blood sugar. We assess prostate health and may recommend bone density testing every 1-2 years if you had osteoporosis initially. Throughout this process, we adjust your treatment based on both lab results and how you’re feeling.
“Monitor testosterone, hematocrit, PSA and prostate examination at recommended intervals,” advise clinical guidelines, emphasizing that regular follow-up isn’t optional – it’s essential.
Our goal isn’t just to get your numbers on a lab report looking good. We want you feeling better, functioning better, and staying healthy for the long term.
Frequently Asked Questions about male hypogonadism
Q: I have fatigue and low energy, but my testosterone level is normal. Could I still have hypogonadism?
While true hypogonadism requires low testosterone by definition, your symptoms might have other causes – thyroid disorders, sleep apnea, depression, or vitamin deficiencies commonly mimic low testosterone symptoms. Another possibility is that your total testosterone looks normal, but your free testosterone (the active form) is low. At our center, we look beyond the obvious, performing comprehensive evaluations to find what’s really causing your symptoms.
Q: Is testosterone replacement therapy a lifelong commitment?
For men with primary hypogonadism (testicular failure) or age-related decline, treatment is typically long-term. However, if your low testosterone stems from reversible factors like excess weight, certain medications, or chronic stress, addressing these issues might restore your natural production. We regularly reassess the need for continued therapy with all our patients.
Q: Can I boost my testosterone naturally without medication?
Several lifestyle changes can help optimize your testosterone levels naturally. Losing excess weight makes a significant difference – each 1-point drop in BMI can increase testosterone by approximately 10 ng/dL. Regular strength training and high-intensity exercise, getting 7-9 hours of quality sleep, managing stress, moderating alcohol intake, and ensuring adequate vitamin D, zinc and magnesium all support healthy testosterone production.
These natural approaches work best for mild cases or as complementary strategies alongside medical treatment. For significant hypogonadism, lifestyle changes alone rarely bring testosterone levels fully into the optimal range.
At the Center for Men’s Health of Rhode Island, we take a comprehensive approach, often combining lifestyle optimization with appropriate medical therapy for the best results.
Conclusion
Male hypogonadism affects millions of men, often flying under the radar while silently impacting quality of life, sexual health, and long-term wellbeing. While testosterone naturally declines as we age, significant deficiency accompanied by troublesome symptoms isn’t something you should simply accept as “getting older.”
Throughout this guide, we’ve covered the essential aspects of this condition, and several important points stand out:
First and foremost, getting properly diagnosed is absolutely crucial. True hypogonadism isn’t just about feeling tired or less interested in sex—it requires documented low morning testosterone levels (below 300 ng/dL on at least two separate occasions) along with clinical symptoms that impact your daily life.
Understanding your specific type of hypogonadism—whether primary or secondary—guides our treatment approach. This distinction helps us determine if the issue originates in the testicles themselves or in the brain’s signaling system.
When it comes to treatment, one size definitely doesn’t fit all. Some men benefit tremendously from lifestyle changes like weight loss and resistance training. Others need testosterone replacement through gels, injections, or other formulations. And men concerned about fertility have specific options that preserve sperm production while addressing symptoms.
The benefits of proper treatment extend far beyond the bedroom. Yes, sexual function typically improves, but men also report better energy, improved mood, positive changes in body composition, improved metabolic health, and stronger bones. Many of our patients tell us they simply feel like themselves again.
Safety remains paramount, which is why regular monitoring through blood tests and check-ups ensures your treatment stays both effective and safe over time. We take this follow-up seriously at the Center for Men’s Health of Rhode Island.
“Testosterone replacement therapy is safe and can be effective for men who are diagnosed with consistently abnormal low testosterone production and symptoms that are associated with this type of androgen deficiency,” states the Endocrine Society, reinforcing our evidence-based approach.
At our center, we specialize in male hypogonadism with a deeply personalized approach. We don’t just measure your testosterone and send you on your way. Instead, we investigate underlying causes, consider your overall health picture, and develop treatment plans addressing your specific concerns and goals.
The fatigue, brain fog, decreased libido, and other symptoms you’re experiencing shouldn’t be dismissed as inevitable parts of aging. With proper care, men with hypogonadism can maintain vitality, sexual function, and overall wellbeing for decades to come.
I’ve seen countless men transform their lives after proper diagnosis and treatment. They return to activities they love, reconnect with their partners, and regain confidence they thought was lost forever.
Ready to take the next step? To learn more about our testosterone testing services or to schedule a consultation, contact the Center for Men’s Health of Rhode Island today. Our experienced team is ready to help you reclaim your energy, vitality, and quality of life.